
What Is Bareback Sex? A Real, Honest Look at the Practice, the Appeal, and the Reality Behind It
Few topics in modern sexual culture stir as much curiosity, debate, and, honestly, confusion as Bareback sex. The term itself […]
Few topics in modern sexual culture stir as much curiosity, debate, and, honestly, confusion as Bareback sex. The term itself […]
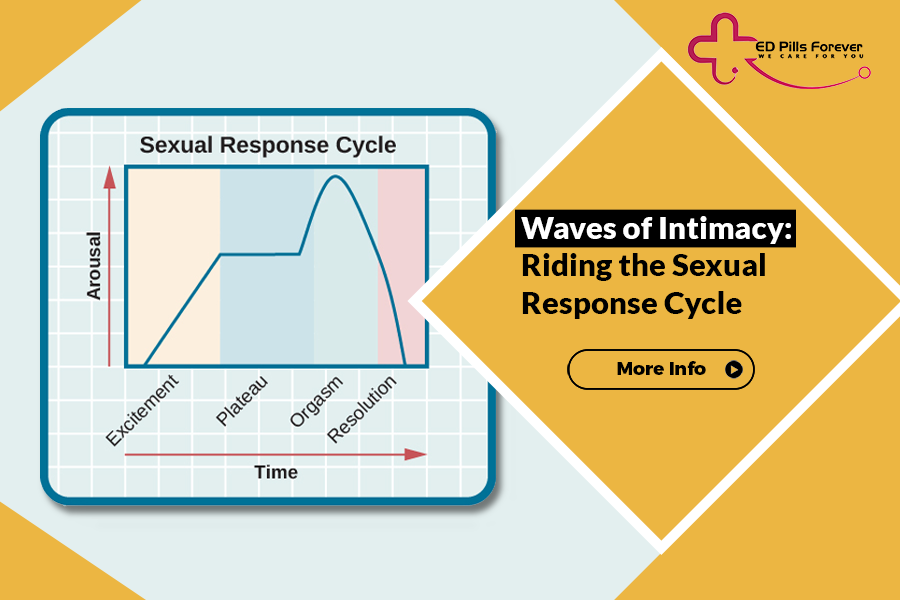
There’s something quietly fascinating about how the human body reacts to desire. It’s not just “get turned on → have
Let’s be real—“Can men have three testicles?” sounds like the kind of question someone blurts out in a late-night group

Erectile dysfunction (ED) is common: stress, poor sleep, vascular health, hormones, medication side-effects, and relationship issues can all play a
Let’s be real, when you hear the phrase how pornography affects real-life relationships, most folks think: “Oh yeah, there must

Let’s be real, people have been getting creative in the bedroom for a long time. From the invention of sex

Let’s be real, if you’ve ever hit the gym hoping for more than just muscle gains, you’re not alone. The

Erectile dysfunction (ED) and urinary problems like frequent urination, urgency, weak stream, nocturia, and overactive bladder (OAB) often show up

Let’s be real, talking about erectile dysfunction isn’t exactly dinner table conversation. It’s one of those topics men often avoid,

Coconut oil keeps popping up in headlines, recipe blogs, and TikTok wellness reels — touted as everything from a kitchen